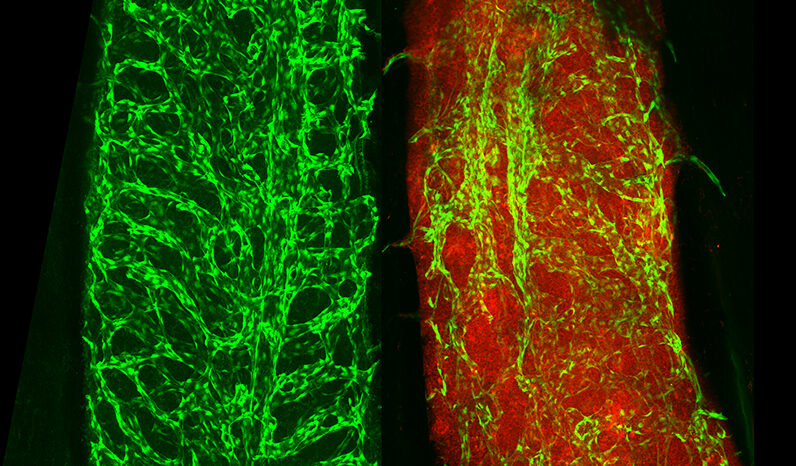
Leukaemia is a cancer of blood cells arising in the bone marrow. Healthy blood consists of many cell types that work together in a balanced system.
In leukaemia, one type of blood cell is abnormal and builds up in numbers. This deprives other cells of the space and nutrients to function properly. Leukaemia develops in the bone marrow, where blood cells are formed. Leukaemic cells can overwhelm normal blood cell formation.
Leukaemic cells can also spread around the body, disrupting the function of other organs.
There are many types of leukaemia. The names of leukaemias can describe features of the disease and its origins. Many leukaemias’ names reflect the normal blood cell types that the leukaemic cells are closest to:
- Lymphoblastic (or lymphocytic) leukaemias resemble immune cells called lymphocytes.
- Myeloid (or myelogenous) leukaemias can have features of ‘myeloid’ immune cells such as neutrophils, or the early developmental stages of red blood cells or platelets.
Leukaemias are often further described by how rapidly the diseased cells are accumulating and worsening the disease.
- Acute leukaemias involve rapidly dividing cells that have features of immature (undeveloped) blood cells. These cells can quickly hinder normal blood cell functions such as fighting infection.
- Chronic leukaemias display a slow accumulation of cancerous cells that resemble more mature blood cells. This can occur over months or years.
In some cases, a leukaemia may begin in a chronic phase but later change, or progress, to an acute leukaemia.
Some leukaemias are very similar to other cancers of blood cells including: