Melbourne researchers have discovered cancer and immune cells rely on the same energy sources from our body to thrive which could trigger a fundamental rethink of treatment options for some lung cancer patients.
The WEHI-led study found a method currently used to treat an aggressive form of lung cancer in clinical trials inadvertently prevents immune cells from protecting the body against the disease.
Mapping the ‘energy fingerprints’ involved, the study indicates treatments that aim to suppress tumour growth while simultaneously boosting the immune system may be counterproductive.
At a glance
Research finds a combination treatment used for lung adenocarcinoma – a common form of lung cancer – may not be beneficial to patients, despite entering clinical trials.
WEHI-led team discovered the combined use of a glutaminase inhibitor and immunotherapy suppressed the activity of both cancer and T cells. T cells are crucial in the body’s fight against diseases like cancer.
Findings could lead to a fundamental change in approach to lung cancer treatments, highlighting the importance of evaluating combination treatments in sophisticated preclinical models before human trials.
Pictured L-R: Associate Professor Kate Sutherland
and Dr Sarah Best
While lung cancer represents just 1 in 10 cancer diagnoses each year in Australia, it continues to be the leading cause of cancer-related death. Lung adenocarcinoma is the most frequent subtype diagnosed in Australia, accounting for 40 per cent of all lung cancers.
Immunotherapy is an emerging form of cancer treatment that boosts the immune system to supercharge T cells – immune cells critical to the body’s ability to fight cancer – and is currently being used to treat many lung adenocarcinoma patients.
Tumours usually rely on an energy source known as glutamate to grow and survive. Drugs known as glutaminase inhibitors have been developed to suppress the growth of cancerous tumours by blocking glutamate from releasing its energy.
A combined therapy currently in clinical trials involves a glutaminase inhibitor and immunotherapy, in an approach researchers hoped would provide dual benefits, by blocking tumour growth and supercharging T cells.
But a new study led by WEHI’s Dr Sarah Best and Associate Professor Kate Sutherland, in collaboration with the Peter Doherty Institute and Agios Pharmaceuticals in the USA, provides a fundamental rethink on whether this combined treatment is beneficial.
The research is published in Cell Metabolism.
Unexpected discovery
Lead author, Dr Sarah Best, said testing the glutaminase inhibitor on preclinical models delivered surprising results.
“We found the drug was not only blocking the activity of the tumour but also the activity of T cells, which are critical to the body’s fight in killing these tumours,” Dr Best said.
“Immunotherapy works by enhancing the activity of T cells. Our findings show the glutaminase inhibitor counteracts the benefits of immunotherapy, because the drug suppresses T cells from functioning and protecting our body.”
Researchers say the findings are critical, given patients in clinical trials are currently receiving this combined immunotherapy and glutaminase inhibition treatment.
“These immune cells rely on glutamate and the activity of glutaminase to thrive just as much as the cancer cells, and our research has shown this metabolic pathway is essential for T cell anti-tumour activity,” Dr Best said.
Energy fingerprints
More than 1 in 3 lung adenocarcinomas have a common cancer-causing mutation in the gene KRAS – a powerful cancer driver.
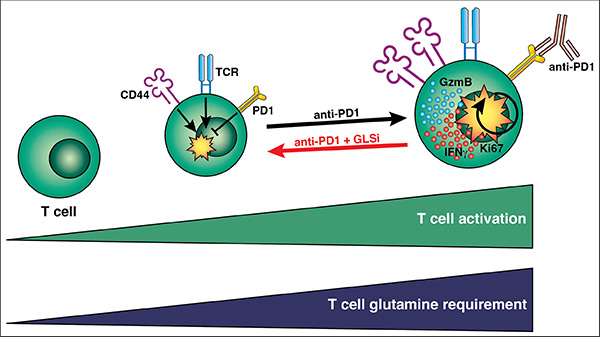
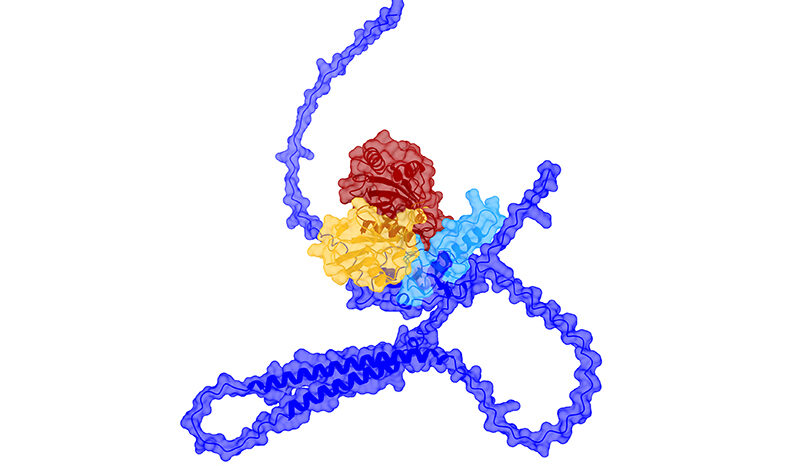
As T cells become highly activated, including by stimulation from immunotherapy (anti-PD1), they rely on the energy source, glutamine, to be fully functional. When their access to glutamine is blocked by a drug known as a Glutaminase Inhibitor (GLSi), they are unable to achieve high levels of activation, and their function is impaired. Credit: WEHI
Associate Professor Kate Sutherland said the new findings built on this research, by showing how unique energy sources fuel the growth of tumours with different co-mutations, known as STK11/Lkb1 and KEAP1. The discovery was made possible by the sophisticated preclinical models used in the study.
“Just like no two fingerprints are the same, we found the metabolite fingerprint of each co-occurring mutation altered the energy usage of KRAS-mutant lung adenocarcinoma,” Associate Professor Sutherland said.
“This matters because the focus until now has predominantly been on key mutations, like KRAS.
“Our work highlights the importance of investigating the other co-mutations without a ‘one-size-fits-all’ approach, because these additional mutations are critical in driving large changes in tumour biology that would impact treatment options and outcomes.”
Researchers say the glutaminase inhibitor could still have benefits for some patients when not combined with immunotherapy.
“We found tumours with the combination of KRAS and STK11/Lkb1 mutations produced elevated levels of glutamate that enable tumours to thrive in preclinical models,” Associate Professor Sutherland said.
“So using the glutaminase inhibitor by itself would be beneficial for patients with this mutation profile. But combining immunotherapy with an inhibitor is unlikely to have positive outcomes.”
The team hopes their work will highlight the importance of considering model systems for examining complex questions on the tumour microenvironment, including metabolic profiles and immune cells. This is especially important when designing complex combination therapies.
The research was supported by the NHMRC, Cancer Australia, the Victorian Cancer Agency, AGIOS Pharmaceuticals and the Peter and Julie Alston Centenary Fellowship.
WEHI authors: Sarah Best, Ariena Kersbergen, Jackson McDonald, Waruni Abeysekera, Alexandra Garnham, Clare Weeden and Kate Sutherland.